- On-Call News
- Posts
- The Deal That Wasn’t: Nodal Pay Reforms Not Enough To Hold off The BMA
The Deal That Wasn’t: Nodal Pay Reforms Not Enough To Hold off The BMA
What was the deal rejected by the BMA committee before it could be given to members?
On-Call News
April 05, 2026

Contents (reading time: 7 minutes)
The Deal That Wasn’t: Nodal Pay Reforms Not Enough To Hold off The BMA
Weekly Prescription
Digital Confessions: Why Patients Tell Machines the Truth
Board Round
Referrals
Weekly Poll
Stat Note
The Deal That Wasn’t: Nodal Pay Reforms Not Enough To Hold off The BMA
What was the deal rejected by the BMA committee before it could be given to members?

Streeting had to circle a new set of dates on his calendar last week. Tuesday 7th of April through to Wednesday the 13th, immediately following the Easter bank holiday weekend. These are the dates the BMA has chosen to apply pressure on the government, armed with a renewed mandate that runs until August 2026 and which passed with a turnout of 53%, just clearing the legal threshold.
There may have been some expectation within government that recent progress on workforce legislation would soften the BMA’s stance. If that hope existed, it has not lasted. This now marks the fifteenth round of industrial action in pursuit of full pay restoration, and the fourth consecutive year in which strikes have formed part of the dispute.
The Rejected Deal
Before turning to opinion, it is worth examining the offer that was ultimately rejected by the BMA committee without being put to members. The Doctors’ and Dentists’ Review Body (DDRB) recommended a 3.5% pay increase. Using CPIH as our marker for inflation, which stood at 3.2% over the preceding year, this would represent a marginal real term increase of 0.3%.
The government’s most recent proposal went beyond that headline figure, however. Its central feature was nodal point reform. At present, recognition of experience within training grades is relatively blunt, with pay often unchanged across multiple years despite increasing responsibility. A CT1 and CT2 are paid the same, as are doctors across ST5 to ST8, despite clear differences in seniority. Streeting proposed reforms aimed to introduce more granular pay progression, affecting both trainees and locally employed doctors.
When combined with the 3.5% uplift, the modelling suggested that foundation doctors would see projected increases of around 6 to 7% by 2026 to 2027, with more senior trainees seeing larger cumulative gains, approaching 9 to 10% in some cases, such as ST5 and ST8 pay. The nodal reform element alone was estimated to cost in the region of £700 million over three years, not an insignificant concession from the government, given the financial climate.
The BMA’s Grievance
The BMA’s official response has been to accuse the government of “shifting the goalposts”, with The Guardian reporting that the union wanted to have all the financial benefits in the 2025/26 year. The reporting in the Guardian states that the government demanded that it had to be over three years to manage affordability. So, it seems that, at its core, the disagreement is not just about the size of the offer, but about timing and perhaps even trust. The longer the timeframe on a deal, the more likely it is for externalities to get in the way of promises.
Beyond pay, the offer contained several measures that are easy to overlook but meaningful in practice. These included reimbursement for mandatory Royal College examinations such as MRCP, MRCS, MRCGP and MRCPsych. The government has also repeatedly committed to increasing speciality training numbers, including an additional 1000 posts from this August and a minimum of 4000 over three years. Yet many applicants going through the current recruitment cycle have struggled to see where these posts have materialised when checking their Oriel accounts…
A Divided Profession
There can be little doubt about how divided resident doctors are on the current dispute. The turnout of the last vote to extend the BMA’s mandate is a testament to that. The latest government offer put to doctors was certainly not trivial but fell short of the BMA’s full pay restoration demand. At the fringes, you will find doctors who believe anything short of FPR entrenches declines, whilst at the other end, some doctors will call it unrealistic and ignorant of current fiscal concerns, which risks eroding our reputation publicly.
Proponents of strike action will tell you that every round of industrial action has brought more generous offers from the government, but waning voter engagement has also shown a more divided profession. To be in medicine in 2026 is to be surrounded by paradoxes. For now, all we can do is wait to see to what extent doctors decide to engage in this round of industrial action.

Lessons From The Oncology Ward: The Burden of the “All-Clear”
After two months of NHS lunches and disrupted afternoon naps, Martin had finished his final cycle of chemotherapy and received the all-clear from the Consultant. He refused to ring the bell on the ward, however; for Martin, the prospect of recurrence was never far from his mind.
“It’s just the way I’ve always been,” he told the medical team. “My mammalian brain can’t help but think of worst-case scenarios. Sitting under the Sword of Damocles... I suppose this is the price one pays for being cured.”
The Sword of Damocles originates from an ancient Greek parable describing a courtier seated beneath a blade suspended by a single strand of horsehair. It tells us how those in positions of success or power often live in a state of perpetual anxiety, shadowed by an impending sense of doom.
In medicine, we can provide patients with figures, data and percentages regarding recurrence risk, but the reality is that no data point can cultivate a tolerance for uncertainty. This is the burden many of our patients carry, yet we often act as though the word ‘cured’ automatically dissolves the discomfort of not knowing what comes next.
Time to develop your teaching skills?

➡️ Want to develop your teaching skills?
➡️ Want to demonstrate your leadership capabilities?
➡️ Want to boost your portfolio?
Medset’s Train the Trainers, Leadership & Management and Human Factors courses are the answers you were looking for…
Online and Live Virtual Classroom options available - use code ONCALL10 for a 10% discount.
Need points for your specialty applications?
Read this guide on scoring points for specialty applications.
Digital Confessions: Why Patients Tell Machines the Truth
Is our profession safe from empathetic AI machines?
As the tentacles of artificial intelligence reach into one profession after another, workers across every sector are grappling with the potential impact on their jobs.
For a long time, doctors have operated under the assumption that the empathetic nature of the clinician renders the doctor irreplaceable. They tell themselves that a cold and callous large language model cannot possibly provide the human touch necessary to navigate a medical encounter.
However, writing in the BMJ, Charlotte Blease reminded the medical community that this premise is simply untrue. There is a robust body of research dating back to the 1960s suggesting that patients often report more candidly to non-human interfaces than to clinicians. This is supported by evidence showing that digital questionnaires can elicit more honest information on sensitive topics such as sexual behaviour, suicidal ideation, and domestic violence than traditional in-person consultations.
AI Empathy Experiment
The On-Call team presented ChatGPT with a vulnerable patient who noticed some blood in their stool and felt embarrassed at the discovery. Chat-GPT responded by stating: “I am glad you spoke up. Whilst embarrassment is common, these are issues doctors take seriously and manage every day.” Come on, how could you not feel more at ease after hearing such a response?
The psychological mechanism at play here is clear because when the perceived risk of judgment is reduced, the level of disclosure increases. This is particularly evident in socially sensitive contexts. As much as we attempt to mould the medical profession into a non-judgmental force through communication skills training and Situational Judgement Tests, we remain human.
Our perspectives are inevitably colored by worldviews, ideological leanings, and past experiences. While most doctors in the NHS understand that personal judgment must be sidelined to ensure a high standard of care, this objectivity is not universal. We also know that humans are uniquely susceptible to the effects of fatigue during shifts and the rigidities of professional hierarchy in their manner and decision-making.
Is The ‘Human-Touch’ a Strength?
We often claim that the human touch makes our profession, well, ‘untouchable‘, yet are we overlooking part of the picture? It is possible that the facelessness and the absence of tone or posture in digital systems actually function as a clinical strength in certain scenarios.
Gemini will not raise an eyebrow at a comment regarding a patient's drinking habits. Claude will not adopt a patronising tone when a patient shares their deepest anxieties. In a recent study involving one hundred and forty-nine simulated primary care cases, patients rated the AI clinician interviewer as significantly more polite and attentive than its human counterparts.
While concerns regarding the privacy of personal information persist, it seems clear that patients will not be ceasing their digital medical conversations any time soon.

A round-up of what’s on doctors minds
“Guys, if you don’t want the med student to follow you to the toilet, tell them where you are going.”
“Some people say that one ‘battles cancer’. As I lay in an NHS side room receiving my treatment, I feel more of a passive host forced to face my enemy. You are less a soldier, than the battleground itself.”
“Hearing a story of a CT1 being pulled from theatre to cover the wards due to staff illness, and a PA being asked to assist the consultant. Yes, the optics of this are awful and unfortunate, but one can see why the decision was made. The CT1 has the capability to look after the ward independently. They can prescribe for a start and likely have the clinical acumen needed to look after a ward of patients unsupervised, unlike the PA.”
“I am genuinely in disbelief that at some point in my weekend shift, I was bleeped to deal with a seagull in the stairwell, and I actually went and dealt with it. Should I fill out a DOPS on Horus?”
What’s on your mind? Email us!

Some things to review when you’re off the ward…
The BBC gave their breakdown of the upcoming round of industrial action by looking at how much resident doctors are paid. Have a look at their analysis here for some numbers.
What do you think NHS chief executives should earn? The NHS is one of the biggest employers in the world, and the top job of a trust is no doubt a stress-inducing job that requires a high degree of competence. But when Hull University Teaching Hospitals Trust and Northern Lincolnshire and Goole Foundation Trust found themselves at the foot of the NHS rankings, their NHS chief executive, Lyn Simpson, found herself at the end of a hit piece by the Times, questioning her £279,000 salary. Here is the full piece.
Weekly Poll

Relative to your grade as a doctor, do you consider yourself adequately paid for the labour that you do? |
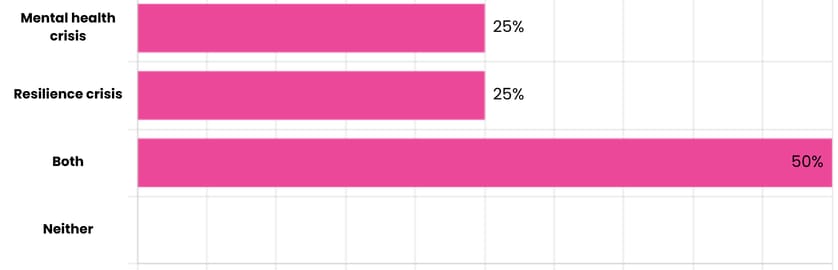
Last week’s poll:
Is Britain facing a genuine youth mental health crisis, or a crisis of resilience?
…and whilst you’re here, can we please take a quick history from you?
Something you’d like to know in our next poll? Let us know!

Some Data on What ‘Well Paid’ Actually Means.
Pay has never been more central to the conversation for resident doctors than in recent years. Round after round of industrial action have sparked intense debate, both on the wards and in the media, over what constitutes "fair" pay. But what does it actually mean to be well-paid? While the answer is, of course, relative to the value of one’s labour, statistics always help ground the discussion.
To define a "high earner," we first need a baseline. The median pre-tax salary for full-time UK workers is approximately £39,000 - a figure every NHS doctor exceeds. If we look at "higher rate" taxpayers (those earning over £50,271), we are looking at the top 18% of the population. Meanwhile, the Office for National Statistics (ONS) defines a high earner as someone making 1.5x the median hourly pay (£26.94 per hour), a bracket containing 23% of workers.
However, "feeling" wealthy is far from universal. In London, reaching the top 1% requires £650,000 annual income, compared to £216,000 elsewhere in the UK. Our social circles and geography heavily dictate our expectations in life, with polling data telling us that Londoners typically believe it takes £289,000 to be considered a high earner, while those in the North set the bar at £80,000. So ‘feeling’ well-off is not universal around the country.
Help us build a community for doctors like you.
Subscribe & Share On-Call News with a friend or colleague!
Reply