- On-Call News
- Posts
- Back to the Picket Line
Back to the Picket Line
What comes next for resident doctors after the passed ballot vote?
On-Call News
July 13, 2025

Contents (reading time: 7 minutes)
Back to the Picket Line
Weekly Prescription
NHS by the Numbers: Spending, Staffing, and Social Care Gaps
Board Round
Referrals
Weekly Poll
Stat Note
Back to the Picket Line
What comes next for resident doctors after the passed ballot vote?
It’s been a tough couple of weeks for the Chancellor, whose attempts to shave £2 billion off the £316 billion social security budget led to division in her own party and uproar in the commons.
She may need to reopen the spreadsheet soon, however, with the BMA ballot results returning a YES vote and a new six-month mandate for industrial action; and the union wasn’t hanging around either, announcing the dates for the walkout just 24 hours later.
The Politics of Turnouts
The ballot saw a 55% turnout, with 90% voting in favour of industrial action. Opponents of strike action have been quick to remind everyone that this amounts to just under 50% of all eligible BMA members. Compile this with the resident doctors who are not BMA members - a group less likely to be supportive of strike action - the proportion of all resident doctors endorsing strike action drops even further. Of course, the specific percentages matter, but more broadly, there is huge political weight in the fact that over 20,000 resident doctors are willing to withdraw their labour over pay.
The obvious rebuttal to government claims of a weak BMA mandate has been the comparison to Labour’s recent general election victory where they received 33.7% of the popular vote on a turnout of 59.7%. Whilst the appeal of this argument is obvious, the comparison seems to be less politically sound. The first-past-the post electoral system, multi-party voting dynamics, protest abstention and a sense of an inevitable Labour victory (which led some voters to stay home), all differ from a binary referendum-style strike ballot. What we generally see (and expect) in politics is that referendums draw larger turnouts, especially when the question can be seen to be of huge personal relevance, such as the Scottish independence referendum which saw an 84.6% turnout.
For those who support strike action, there are legitimate reasons for dissatisfaction that a previous generation of doctors may not be able to empathise with. These doctors worked at a time where tuition fee repayment was not a concern, hospital accommodation was subsidised during the house officer years, the housing market wasn’t in crisis and speciality bottlenecks were not as severe as today.
Define ‘Real Terms’ Fall
Central to the pay dispute is how inflation is measured and what constitutes a "real terms" fall in pay. We recently did a deep dive into the debate between the use of RPI (retail price index) versus CPIH (consumer price index including owner occupiers’ housing costs). The Institute for Fiscal Studies (IFS) and Office for Budget Responsibility (OBR) have both criticised RPI as outdated and economically flawed, yet the government still selectively uses it in certain areas such as student loan interest calculations, a move repeatedly criticised by both bodies.
CPI is used for state pension increases, benefits and tax credits and of course, public sector pay guidance. Maybe the government are finally listening to the IFS as they recently told the UK Statistics Authority they plan to phase out RPI by 2030.
Using CPI, resident doctors’ pay has still fallen, but by a more modest 4.7% since 2008. A look across to the private sector tells us that average earnings here have risen over 7% in that same period, deepening the sense of disparity.
The Cost Of Striking
There can be no doubt that industrial action deals a serious blow to the government. Cancelled operations, delayed outpatient clinics and funding for locums and consultants to cover gaps will cost billions. The government may try to project calm to the media, in an attempt to signal control, but the economic impact of strike action is serious and the government will be well aware of it.
We know that these economic ‘calculations’ are tough to compute whilst taking account of all the externalities. However doctors may claim that if salaries do not reflect their professional value, the long term cost of workforce attrition, vacancies and a reliance on locums will come at an even higher price for the government.
Are Doctors Missing The Economical Picture?
Still, it is fair for one to ask whether some resident doctors truly appreciate the broader fiscal constraints facing the country. The OBR’s official forecast this week made for worrying reading. A quick read through will tell you that the the UK has the one of the highest deficits in the world and our national debt sits at 100% of GDP, driven primarily through greater government spending.
The governments recent U-turns on disability benefits and winter fuel payments, compiled with the commitment to the triple lock state pension has made most economists agree that increases in one or more of the three main taxes (income tax, national insurance, or VAT) is inevitable in the next budget.
There will be doctors who care very little for the ‘economic picture’ painted above. Shrugging it off as not their responsibility. This line of reasoning is, frankly, misguided. The UK’s fiscal health matters, not only to the NHS, but to everything from the taxes we pay, our mortgage rates, to the society our children grow up in.
Doctors should absolutely advocate for fair pay, but they must also engage with the real economic conditions that determine what is politically and financially possible. As former BMA co-chairs Dr. Rob Laurenson and Dr. Vivek Trivedi noted, full pay restoration was always going to be a journey given the economic climate facing the country. The real question for doctors now is: how long are they prepared for that journey to take?
As both a workforce and a public-facing profession, we must hold two ideas in balance: that doctors have been undervalued, and that our demands exist within a strained fiscal environment. Pretending otherwise weakens our credibility, both with the government and the public we serve.

Young Consultant, Huge Questions: Is 32 Too Young?
You realise early on that medicine is your calling and make it to medical school. The early years as a doctor go by quickly as you pass through the hurdles immediately and suddenly you arrive to the end of training. Shortly after your 30th birthday, you face the prospect of becoming a Consultant.
Some doctors, however, find themselves wondering whether there are any disadvantages of being a young consultant that need to be offset by extending their training.
Let’s put aside the long term financial implications (to your salary and pension) of remaining at senior registrar level for a moment. The On-Call team want to ask you: Was there any level of your training where you did not contend with imposter syndrome?
On the first day as an F1, SHO, or Registrar? We should have enough faith in our training system to say that it is not down to luck that we arrived to the end of training, but skill and hard work?
We do not want to be accused of making the same superficial and blanket statements that we advocate against here at On-Call. After honest reflection in their own practice, a small number of doctors will perhaps find that they genuinely need the extra time to sharpen up their skills and that’s perfectly fine.
However, if the concerns lie around management, politics and dealing with secretaries and general managers, everyone practically starts from the same point whether you become a consultant 32 or 55.
NHS by the Numbers: Spending, Staffing, and Social Care Gaps
Essential insights into where we stand — and where the pressure points lie.
If someone asked whether you are up to date with the facts about the NHS, what would you say? In an age of sexed-up anecdotes, social media and fake news, it has never been more important to have accurate information. Fortunately, we have some essential data from the team at The Kings Fund, so you don’t have to guess.
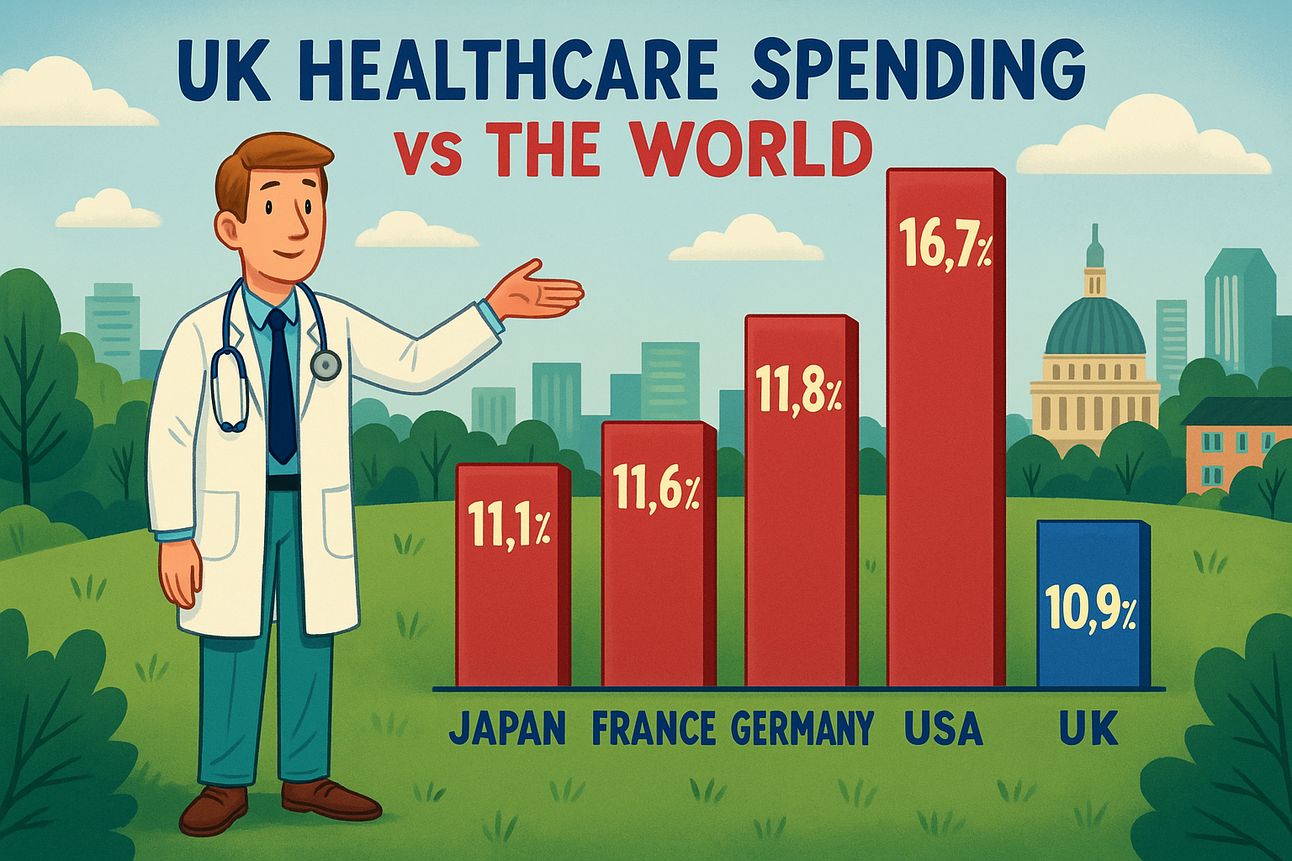
UK Healthcare Spending vs The World?
What percentage of our GDP do we spent on healthcare compared to other comparable nations? Have a think… If you answered close to 10.9% then congratulations.
This is fairly comparable to countries in the EU15, G7 and Anglosphere with the only countries lying ahead of the UK being Japan (11.1%), France (11.6%), Germany (11.8%) and the USA out ahead at 16.7%. Although our friends from across the pond may spend more, don’t mention any issues with equity or access of care…
If we shift to spending per capita, the picture is less favourable for the UK. The UK spends around €3,651 per person on healthcare (apologies, the data was in Euros), far below Norway’s €5376 and Germany’s €5317. We need to be careful however - more money doesn’t necessarily lead to better healthcare. Taking one metric of preventable deaths per 100,000 people (defined as deaths that could have been avoided through timely and effective healthcare), Germany’s 171 preventable deaths is higher than the UK’s 167. So these calculations are complex and it’s never quite as simple as more funding equalling better, more affordable care.
Cost of an A&E Admission?
What does an Accident & Emergency admission actually cost? Of course this depends on the urgency of the admission and the type of care you require. At the lowest level of investigation and treatment you are looking at a bill of £114 per attendance, with the average cost of a patient taken to A&E in 2023/24 being £459.
Rank by Number of Staff: Doctor, Nurse, Allied Health Professional
Our nursing colleagues take the top spot with a total of 392,800 staff in the NHS. This is followed by the 199,200 allied health professionals and 147,300 NHS doctors. If we want to focus on growth, between 2010 and 2025, the largest increase in staff numbers have been doctors, whose numbers increased by 54% in that period, compared to a 31% increase in nurses and a 45% increase in allied health professionals. The number of managers has increased 6% in that time. Despite the increase, as of March 2025, the NHS estimates there are 7,700 vacancies in doctor roles.
How many People in the UK receive social care?
2023/24 saw over 2 million applications from new clients asking for support. 658,000 of these were from working age adults. 42% of requests resulted in some form of service, usually through publicly funded long term social care in residental/nursing homes or within their own homes. 27% received advice or signposting and the remaining 31% did not receive anything. With that number nearly totalling a third, we can see there is a significant unmet need for social care.
It should be no surprise that the rise in social care requests is being driven by patients living longer with more complex health needs and our over 85 population is set to grow by over 100% in 2050.

A round-up of what’s on doctors minds
“Has anyone thought about what this new ‘patient satisfaction’ rating system means for pathologists and radiologists? No 5 star ratings but no 0 star ones either I suppose”
“I can’t wait to read some of the ITU patient satisfaction reports: When our gran, Mavis got admitted to hospital aged 98 with 3 stents and one functioning kidney, we were really disappointed that the ITU team gave up on her and said following a review that they wouldn’t be taking her to intensive care. It’s just not the standard of care one would expect from the NHS - 0 Stars”
“Good locum rates and London can never exist in one sentence (unless your on first name basis with the Consultant from the golf club).”
“1 billion pounds would fund the NHS for 2.1 days”
What’s on your mind? Email us!

Some things to review when you’re off the ward…
Has science found the answer as to why boys are three times more likely to develop ADHD than girls? Academics from the University of Rochester seem to think so.
You may remember that in December 2024, the government introduced GP reforms to reduce the number of performance target’s that GPs must meet. Despite this, there are still countless GP target’s. If you are interested in seeing all of them check out page eight of this NHS England document.
Weekly Poll
Would you be comfortable being one of the NHS’s young consultants at 32 years old?? |
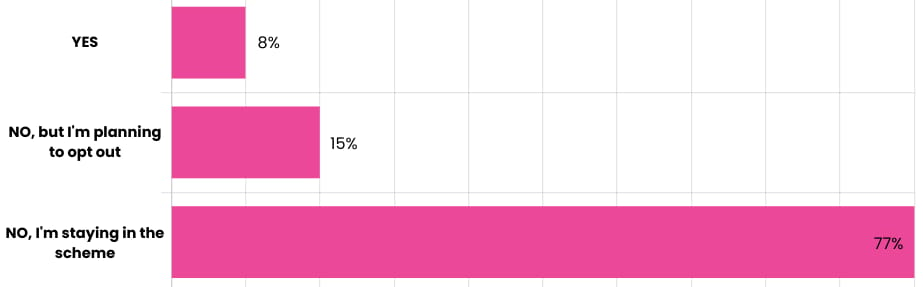
Last week’s poll:
Have you opted out of the NHS pension?
…and whilst you’re here, can we please take a quick history from you?
Something you’d like to know in our next poll? Let us know!

50-50: Is a Limited Company The Answer For Consultants?
As the government makes another financial U-turn, Speculation grows amongst economists and political pundits that Rachel Reeves’ will be preparing another flurry of tax-rises in the next budget. The On-Call Consultant community look on, already feeling disillusioned by the frozen tax thresholds, child benefit withdrawal, the £100K tax trap and pension tapering.
Some may be considering channelling private income through a limited company. The logic being that their income would be taxed at lower corporation and dividend rates, rather than the higher personal income tax bands. The guys at MedicsMoney found that approximately 50% of doctors would benefit from this financially.
Why? Well, limited companies come with additional costs (and grey hairs) through annual accounts, corporation tax filings, bookkeeping and accountancy fees. It’s not the cost you just have to worry about either, the time expended could be spent working or spending time doing what matters to you in life. It’s also worth considering that this income will not contribute to NHS pension benefits, and pension contribution would have to come through a Self-Invested Personal Pension (SIPP).
Crucially, IR35 (one of the many pieces of UK tax legislation) rules apply. If you’re working like an employee, (through working NHS locum or bank shifts) you are inside IR35 and HMRC requires PAYE and national insurance tax treatment. Since 2017, NHS trusts have been assessing IR35 status closely. Locum work should therefore not be funnelled through a limited company to pay lower rates of corporation and dividend tax.
Help us build a community for doctors like you.
Subscribe & Share On-Call News with a friend or colleague!
Reply